Trans-catheter Aortic Valve Replacement (TAVR) Program
Trans-catheter aortic valve replacement (TAVR) is a minimally invasive (percutaneous) procedure used to replace a blocked aortic valve (aortic stenosis). This procedure is often called TAVI (trans-catheter aortic valve implantation).
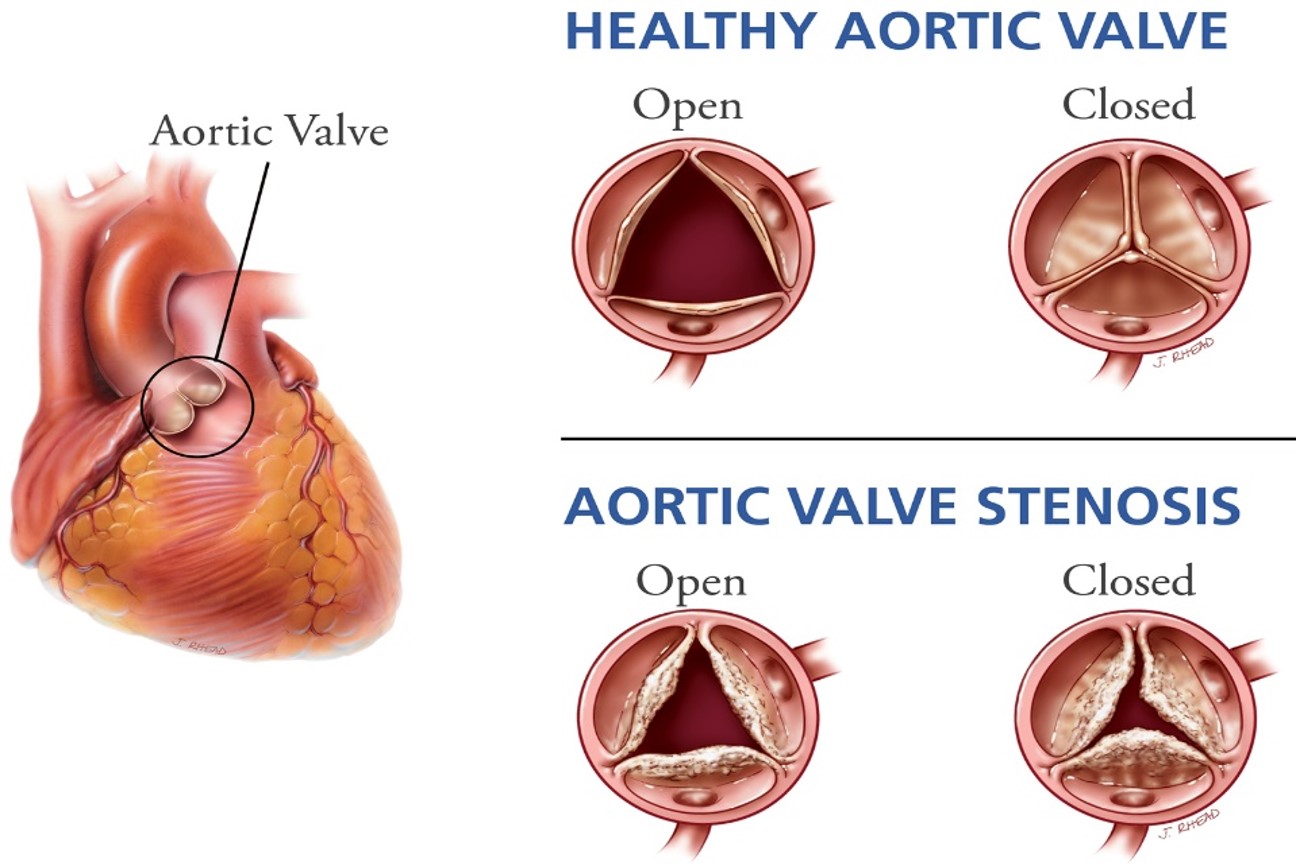
Aortic valve stenosis (AS) develops when the aortic valve narrows due to scarring and calcification. The decreased mobility of the valve components (leaflets) results in obstruction of the blood flow and lower perfusion of the rest of the body resulting in the classic symptoms of fatigue, chest pain, shortness of breath and eventually sudden death. As the aortic valve orifice decreases in size a murmur develops.
TAVR and surgical valve replacement (SAVR) both relieve the symptoms associated with aortic stenosis and prolong survival. TAVR is an alternative treatment option to open surgery in patients with AS who are calculated at moderate and high risk for operative mortality and major complications. TAVR is often indicated in patients that can’t undergo SAVR for technical reasons, frailty or advanced age.
Patients who benefit the most from this procedure are usually elderly (75 and older), had previous surgery, are frail and have multiple other medical problems. The calculated STS surgical risk (Society of Thoracic Surgery risk calculator) is usually greater than 2 %.
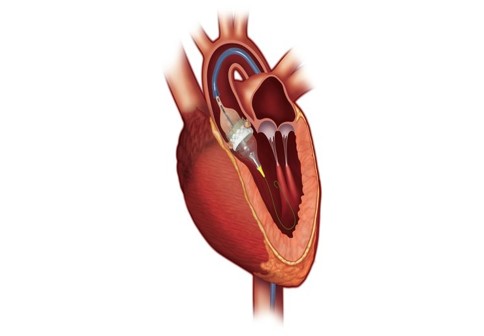
TAVR is predominantly performed through a puncture or small opening in a groin vessel. Less commonly, access has to be obtained through the apex of the heart (small incision between the ribs), main aorta, carotid artery or an arm vessel. The crumped valve is advanced under fluoroscopy guidance inside the blocked valve and then a balloon is inflated to deploy the stented new valve inside the diseased one. The heart is transiently stopped or rapidly paced during the deployment (10-20 seconds).


Although the risk of the procedure is very low, there is a procedural mortality of 1-2 % and complications include bleeding, stroke, groin vessel rupture, kidney disease, infection and technical issues related to valve positioning such as leaks, misplacement and heart block often requiring a pacemaker (5%). Occasionally, the procedure needs to be converted to open surgery (< 1 %).
Before TAVR is indicated, you will need to be evaluated extensively by a multidisciplinary team of cardiac surgeons and cardiologists and multiple tests including an echocardiogram, cardiac catheterization and computed tomography will be required. The team will evaluate your particular condition to determine the most appropriate treatment in your case. The indication for TAVR is not a patient preference but a medical decision based on objective clinical data, physician judgement and present CMS (Center for Medicare Services) guidelines, and will require your insurance approval.
Our TAVR program started in 2014 and has nearly 1000 cases performed. Our success has been based on strict patient selection, adherence to present guidelines and very detailed procedural technique. This approach has resulted in excellent outcomes with very low complication rates and great patient satisfaction.
Call our TAVR program – Cardiac Surgery at Baptist Health Louisville for an evaluation or second opinion for aortic stenosis or heart murmur at 502.893.3021 and 502.899.3858