Hello, my name is Doctor. Lanny Gore and I'm a bariatric surgeon at Baptist Health Floyd in New Albany, Indiana. I am board certified and a fellow of the American College of Surgeons and a fellow of the American Society of Metabolic and Bariatric Surgeons.
Through bariatric surgery, we can treat multiple medical problems by focusing on obesity, which is often the root of the problem. Bariatric surgery is safe and more people in our community need it to overcome obesity.
We are fully committed to making your treatment a success.
We start by asking you about your goals and your challenges so we can recommend the treatment that works best for you.
Today we'll talk about the implications of obesity, including the comorbidities or diseases obesity causes.
And we'll talk about the different procedures and the different tools that we offer.
At the end of the presentation, you can begin your journey to surgery.
So what is obesity? Obesity is a genetically related and costly, multifunctional disease of excess fat storage with multiple comorbidities. It's lifelong, it's progressive, and life threatening. Morbid obesity is the point at which serious medical conditions occur as a direct result of the obesity.
Next we'll show a video about set point range. According to the set point range we all have a metabolic range of weight that our bodies want to maintain. This could be one hundred pounds or two fifty pounds or anywhere in between, But our body wants to be at that weight.
We have become obese as a society because of the Western diet and specifically American food. Companies have taken all the nutrients out and left us with all the calories. Additional causes of obesity in modern society include certain medications, lack of exercise, lack of sleep, and stress.
The Set Point Theory suggests that no matter what you want to weigh, your brain has a certain weight range and body level that it works to maintain within the set point range. This means that you don't control your body fat consciously, rather your brain manages it like it does your breathing and heart rate. Your brain receives information through hormone signals from your body fat, muscles, pancreas, liver, GI tract and sensory organs at all times and controls your appetite, digestion, energy balance and metabolism.
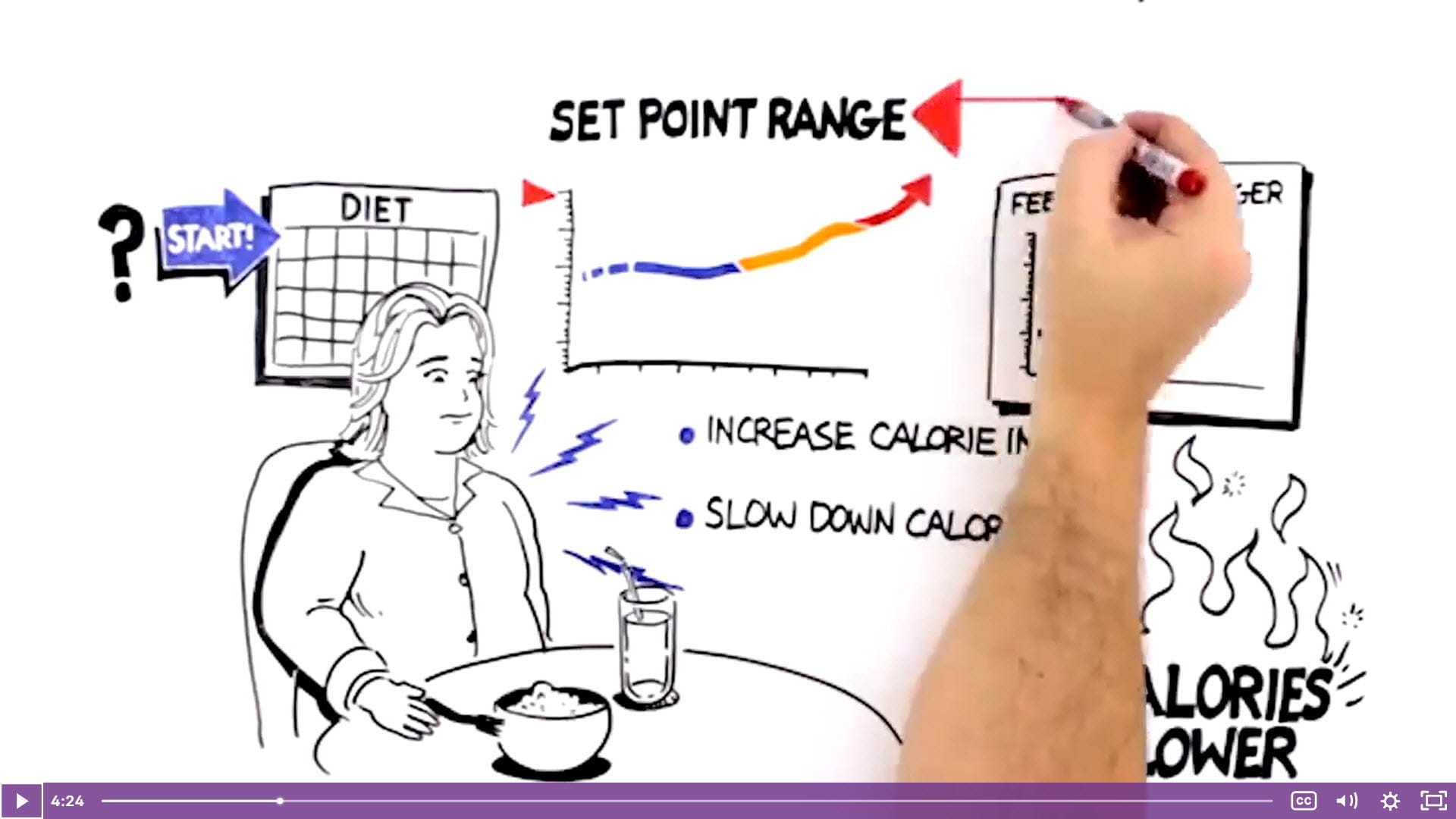
Once your set point has been elevated, your body works to defend it vigorously. What happens when Amanda starts a diet? She might be able to lose some weight temporarily, but hormone signals from her body change in response to weight loss and tell her brain to increase calorie intake and slow down calorie burn to restore the body fat she's lost. She feels hungrier, and although she doesn't know it, she's also burning calories slower than before.
Amanda's body doesn't recognize that her set point is too high and her weight is unhealthy. It only knows to defend her current set point.
What that video was trying to show us is that we all have a set point weight that our body wants to maintain, and when we lose weight, our bodies see that as abnormal.
And it's going to do whatever it can to drive it up to that metabolic set weight point that our body wants to be.
There are degrees of obesity, and we can give this degree of obesity a number called the BMI.
This is what the insurance companies look at to see if you qualify for surgery, and what that stands for is body mass index, and it's actually a height and weight calculation.
The normal patient has a BMI of eighteen point five to twenty four point nine.
An overweight individual may have a BMI of twenty five to twenty nine point nine. And then the weight loss surgery patient has a BMI of thirty or greater.
Insurance companies look at these categories at the end here, BMI forty and above.
Most insurance companies will cover that without any type of other requirement unless there's an exclusion in the insurance policy.
But with a BMI of thirty five to thirty nine point nine, most insurances require some type of comorbidity like hypertension, type two diabetes, or sleep apnea before they would approve the surgery. And at the present time, we are starting to see some insurance companies cover bariatric surgery for a BMI as low as thirty with a disease like type two diabetes or liver disease.
Here are two maps showing the percentage of obesity in adults in the United States.
As you can see, in twenty eleven, in Kentucky and in Indiana, the rate of obesity was thirty to thirty five percent and then rose in twenty nineteen to greater than thirty five percent.
You can also see that these states were among the states in the nation with the highest rates of obesity.
One in five deaths of African Americans and Caucasians age forty to eighty five is attributed to obesity.
It is second to only smoking as the leading preventable cause of death. It contributes to heart disease, cancer, and diabetes, and many others.
There's also a social impact of obesity. It's still a form of social discrimination.
There's a lot of fat shaming in our society, and there's even discrimination in the workplace. You'll have limited recreational opportunities, such as difficulty flying in a plane or going to a movie.
So what are comorbidities of obesity?
These are medical problems that are related to obesity. Diabetes, especially type two diabetes, is very much affected by obesity. High blood pressure is a common thing we see among our patients.
Obstructive sleep apnea is very common. Fatty liver disease and other problems that affect women such as infertility, polycystic ovarian syndrome, and obstetric complications are common.
Obesity can even increase your risk of cancer.
Some of these include esophageal cancer, endometrial colon cancer, gallbladder cancer, cervical cancer, breast cancer, skin cancer, ovarian cancer, and kidney cancer.
Patients with severe obesity who have bariatric surgery lower their risk of developing cancer by at least one third.
The weight loss procedures that we offer at Baptist Health include the gastric sleeve or vertical sleeve gastrectomy, Roux en Y gastric bypass, and also the new endoscopic sleeve gastroplasty and one anastomosis gastric bypass. We also do many revision procedures as well.
Now we used to think of bariatric surgery as just restrictive or malabsorptive type procedures, but actually data suggests that it's actually a metabolic or physiologic procedure, meaning that there's a change in how these hormones are being signaled to our brain and how we lose weight. So it's not that we just decrease the amount that we are able to eat in one sitting or that we don't absorb as much calories. It's actually changing hormones and how they're being signaled to our brain.
The first procedure we're going to discuss is the gastric sleeve or vertical sleeve gastrectomy. In this procedure, we remove about seventy five percent of the stomach. So instead of having this big football sized stomach, we have a banana sized stomach. We remove the top portion of the stomach called the fundus, which produces the majority of the hunger hormone called ghrelin. That's why sleep patients do have a decreased hunger sensation or decreased appetite because of this procedure. Again, it's a metabolic type procedure. This procedure takes about thirty to forty five minutes to perform, all done through minimally invasive small incisions, which we'll show you in a minute.
The stomach that remains is about the size of a banana, as I said. And again, we're reducing the ghrelin hormone.
The majority of that is taken out by removing the fundus portion of the stomach.
To access the abdominal cavity, small incisions are created. Trocars are placed to serve as passageways for surgical instruments.
The surgeon examines the abdomen using a laparoscope or video camera. The average human stomach can expand to hold around one to one point five liters of food. While in the stomach, food is combined with digestive enzymes. These help break the food down into a simpler form so that it can be digested more easily and absorbed in the small bowel.
During a sleeve gastrectomy, a thin vertical sleeve is created by using a stapling device. This sleeve will typically hold between fifty and one hundred and fifty milliliters and is about the size of a banana. The resected portion of the stomach is removed. By altering the anatomy of the gastrointestinal tract, sleeve gastrectomy changes signals in the body resulting in decreased hunger and increased feelings of fullness after meals.
Vile and pancreatic fluid from the liver and pancreas mix with food and allow it to be completely digested and absorbed in the bowel.
There is no rerouting of the small bowel or postoperative adjustments needed for the sleeve gastrectomy.
Let's talk about the advantages and disadvantages of gastric sleeve. Advantages are its rapid weight loss And also, there's no surgical connection or anastomosis that is made when we're performing this operation. You can take about any medication or have any procedure you need to have in the future. It's faster diabetes improvement and resolution.
There's also a loss of hunger with gastric sleeve, a loss of appetite, because we're taking out the part of the stomach called the fundus.
There's no dumping syndrome like we see with other procedures. There's no foreign body.
And basically, this is a good procedure for the majority of patients. The sleeve is considered one of the safest, better procedures after the initial operation is over.
Disadvantages. There's not a lot of disadvantages, but it is a good idea to not take nonsteroidal anti inflammatory medications for a few weeks after surgery. After about a month after surgery, you can take those medications. These medications include things like ibuprofen and Aleve and other NSAIDs. The gastric sleeve is not recommended if you have Barrett's esophagus. The gastric sleeve can increase reflux in some people. So if you have severe reflux, you may want to consider not having a gastric sleeve.
The next procedure I'd like to talk about is the Roux en Y gastric bypass. It is a combination of restriction and malabsorption. In this procedure, we're creating a very small stomach called the gastric pouch and then connecting it to part of the small intestine that is normally found much further downstream.
Now we're going to watch a video showing how the gastric bypass is performed.
To access the abdominal cavity, small incisions are created. Trocars are placed to serve as passageways for surgical instruments. The surgeon examines the abdomen using a laparoscope or video camera. The average human stomach can expand to hold around one to one point five liters of food. While in the stomach, food is combined with digestive enzymes. These help break the food down into a simpler form so that it can be digested more easily and absorbed in the small bowel.
During a gastric bypass, a small pouch is created in the stomach using a stapling device. The small stomach pouch, about the size of an egg, limits the amount of food you can eat before feeling full. The small bowel is separated into two sections. The lower portion of the small bowel is attached to the newly created stomach pouch.
This allows food to pass directly into the second portion of small bowel where digestion continues. The upper portion of the small bowel is reconnected to the lower. Bile and pancreatic fluids from the liver and pancreas allow food to be digested completely. By altering the anatomy of the gastrointestinal tract, gastric bypass changes signals in the body resulting in decreased hunger and increased feelings of fullness after meals.
So what are the advantages and disadvantages of gastric bypass?
Well, the big advantage is very rapid weight loss. There's good long term weight loss from gastric bypass. There's a loss of hunger for an average of six months after gastric bypass.
There is excellent diabetes resolution. There's no foreign body issues or the need to make any kind of adjustments. And it's really the best procedure for patients with Barrett's esophagus or significant reflux.
It's also a very good procedure for patients with severe insulin dependent diabetes.
The disadvantages of gastric bypass is that there's something called dumping syndrome, which is when a patient eats a high sugar meal, he or she may have some abdominal cramping or even diarrhea. A big disadvantage of gastric bypass is that there is a risk of an ulcer. This is called a marginal ulcer. And there's actually about a five percent risk of getting a marginal ulcer. So it's very important not to smoke if you have gastric bypass. It's also very important not to take NSAID drugs like ibuprofen and Aleve.
And it's really important that you never do that for the rest of your life. There's also a risk of a type of bowel obstruction called internal hernia. And so we wanna look out for that and make sure that if you ever have any abdominal pain or symptoms that you see your bariatric surgeon.
Also, there's a significant rate of vitamin and mineral deficiency. If you have gastric bypass, it's very important that you take vitamins for the rest of your life.
There's also a type of a procedure that sometimes is performed called an ERCP, and it's very, very difficult to perform an ERCP in a patient with gastric bypass. The next procedure I'd like to talk about is something new. It's the endoscopic sleeve gastroplasty, or ESG.
It's a procedure that is done not with any incisions in the abdomen. A scope is placed in the mouth and a device is used to make stitches in the stomach to fold the stomach onto itself. This results in a smaller stomach leading to smaller portion sizes.
And this is a good option if your insurance does not cover bariatric surgery or if you have a BMI that's a little lower, like a BMI of about thirty to forty, this could be a good option for you.
This procedure, for those of you that are having to pay out of pocket for it, is much cheaper than traditional surgery. It is possible that coming up in the near future, insurance companies will begin to pay for ESG, so we may see this become a procedure that's performed a lot more frequently in the future.
Another new procedure I'd like to introduce is the one anastomosis gastric bypass. This is a new version of gastric bypass that is simpler and has been shown to be just as effective as traditional Roux en Y gastric bypass for weight loss.
It's a relatively new procedure that was endorsed last year by the American Society of Metabolic and Bariatric Surgeons. It has been performed outside the United States over the past decade and there have been good results for weight loss and resolution of type two diabetes comparable to Roux en Y gastric bypass and sleeve gastrectomy, with some studies even showing superior results.
The operative time for OAGB is relatively short with low complication rates.
There is still risk of marginal ulcer like gastric bypass, but lower risk of internal hernia like with gastric bypass.
There is an increased risk of bile reflux and there is also risk of nutritional deficiencies like Roux en Y gastric bypass. Here's a video showing how one anastomosis gastric bypass is performed.
Small incisions are created for placement of trocars, which provide access to the abdominal cavity and serve as passageways for surgical instruments.
The surgeon examines the abdomen using a laparoscope. The average human stomach can expand to hold around one to one point five liters of food, while in the stomach food is broken down when combined with digestive enzymes so its nutrients can be absorbed in the small bowel. During a one anastomosis gastric bypass, a surgical stapler is used to create a pouch at the top of the stomach. The small pouch, about the size of a small banana, limits the amount of food you can eat before feeling full.
Next, a one hundred and fifty centimeter to two hundred centimeter segment of small bowel to be bypassed is measured off.
A loop is brought up and connected to the newly created pouch through a sutured or stapled connection called an anastomosis.
Bile and digestive fluids from the liver and pancreas allow food to be digested completely.
By altering the anatomy of the gastrointestinal tract, gastric bypass changes metabolic processes and signals in the body, resulting in decreased hunger and increased feelings of fullness after meals. Compared to a traditional gastric bypass, the one anastomosis gastric bypass is typically a shorter and simpler procedure that involves a slightly larger stomach pouch and may require less mobilization and manipulation of the small bowel. And unlike traditional gastric bypass procedure with two anastomoses, it requires the creation of only one.
We also do revisional surgery. If you've had a history of bariatric surgery and have regained your weight or you're having any kind of difficulty in any way, we want to help you manage that.
This might involve converting one procedure to another or revising the procedure that you have already had.
Eating after bariatric surgery starts with liquids and protein supplements so that you slowly add foods until you reach a normal way of eating at about five or six weeks after surgery. Most people want to know when they can return to work or how long you're in the hospital for.
Most of these procedures, it's one night in the hospital and you go home the next day. With the ESG procedure, you likely would just go home the same day.
Most people can return to work in one to two weeks, just depending on how strenuous your job is.
So how do you know what operation is right for you? We want to help you make that decision. I think a discussion with your surgeon is the most important thing when it comes to making a decision about which operation is right for you.
You do have to take into consideration your medical problems when deciding how aggressive you need to be with your decision. And you also should look at the success rate and the complications in order to make an informed decision.
We can help you do that. You can also look at other avenues like support groups that we can help you get involved with. We have our own and there are certainly great ones out there where you can look at other patients' experiences and see what they are going through and see what works for them.
So earlier in the presentation, we talked about comorbidities and how there's all these medical problems that are either exacerbated or even caused by obesity.
The good news is that by treating the obesity, we can see a resolution in these medical problems. We can see people have improvement in their diabetes. They can get off insulin. They can get off their diabetes medication. They can get off their blood pressure medication. Other medical problems like polycystic ovarian syndrome, joint pain, sleep apnea, GERD, hypercholesterolemia, and a lot of other medical problems are significantly improved with weight loss through bariatric surgery.
Now all of our surgeries are done through small incisions using robotic laparoscopic surgery.
We have a comprehensive program that takes place before your surgery and after your surgery. Patients go through an extensive education process.
We are an accredited center by the MBSACWIP. This is a division of the American College of Surgeons, And every three years, program is evaluated and they inspect our hospital and all of our operations to ensure quality. So you can rest assured that we have a good quality program that lives up to the standards of the MBS AQIPP. Now let's hear from some of our patients about their success with our bariatric surgery.
I started at two thirty eight pounds and I'm at one hundred and forty four pounds, so I've lost ninety four pounds.
My weight was knocking on the door four hundred pounds.
And now my weight is down to two seventy pounds and it's just been a tremendous difference.
I tried different things, know, the typical diets, know, this kind of diet, that kind of diet, and nothing was working. So, know, you hear things about bariatric surgery, start researching it, you see that there are favorable results to have.
One thing that I really like to do now is, I have a three and a half year old daughter that loves to play with puzzles. She'd rather play with puzzles than toys. And she'd get on the floor and before surgery she would ask me, know, daddy, can can we build some puzzles? And I'd have to do it at the table.
Well, didn't want to do it. She's two and a half at the time. She didn't want to do it at the table. And I didn't want to do it on the floor because it was hard for me to sit on the floor.
Now we lay on the floor, sit on the floor and build puzzles all the time. And that's great.
I lost fifteen pounds prior to surgery, so I was two fifty five pounds before my gastric bypass. To date, I've lost a total of two hundred pounds, so I weigh one hundred and seventy pounds now.
I've tried to lose weight thousand times. I've been on many programs, many organized programs and many unorganized programs. Before surgery, weighed three forty two pounds and as of today, I'm one hundred ninety one. So I've lost approximately one hundred and fifty pounds.
We have changed the way we eat in many ways and we're eating much, much healthier. Having this surgery is not the end. The surgery is a tool and I can use this tool with my other efforts to be at a weight where I want to be. I probably added ten years to my life by losing one hundred and fifty pounds.
And so that's something that's good to hear because I want to be around for a lot longer.
This concludes our presentation. Thank you very much for your time. We'd be happy to answer any questions you have regarding your weight loss journey and talk to you more about an option that's right for you. Our goal is to provide expert quality care centered on you. Thank you, and we look forward to creating a healthy partnership with you.





.jpg?rev=22e81ba50e9940bda5e9fb2eebbea222)

.jpg?rev=f8343482c79c4e7186c08e46c298b3c6)